

Feeding Therapy Insight
As a pediatric speech-language pathologist with special interest in feeding and swallowing disorders, I have encountered a wide range of ages of children who present with difficulties surrounding feeding and mealtimes for a variety of underlying reasons. I have also had the unique opportunity to see these children make incredible gains and progress toward enjoying mealtimes.
For most of us, eating is generally an enjoyable, fairly effortless experience that we look forward to; but unfortunately this is not the case for everyone.
Prevalence
Studies have shown that 25% of the pediatric population exhibits moderate to severe food refusal and that number increases to 80% in children with developmental delays.

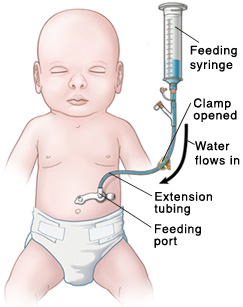
Infants or Children Who are Tube-Dependent or Have a Complex Medical History that Negatively Impacts Feeding
Feeding disorders can present themselves in a variety of ways, making it important to know when your child would benefit from seeing a speech language pathologist who specializes in feeding.

-
Is your child’s medical history significant for complexities that negatively impact their ability to receive nutrition orally?
-
Is your goal for them to rely less on a feeding tube or to decrease building stress when it is time to eat?
When children require significant medical attention, they can develop negative associations surrounding feedings or even any touch close to the face.
Feeding tubes can be required for a variety of reasons, but a speech-language pathologist is knowledgeable on the anatomy and physiology of the systems that work together for eating and drinking and can help you reach goals you have for your child, whether it be related to behaviors, oral motor difficulties, etc.
Enteral feeds can feel unnatural and frustrating for both parents and their children and unfortunately removal can feel like an intimidating and sizable goal. For this reason, feeding specialists also use strategies to make this experience positive, while gaining the child’s trust to allow touch to the face or for foods to enter the mouth without heightened fear that someone is going to hurt them.
The future is always in mind, as we work with families to establish positive feeding behaviors that will decrease stress further down the road. Since caregivers are with their children for the majority of these feedings, it is also critical that the feeding specialist work alongside families as members of the team.










